.jpg)
Living with chronic pain often means living with unanswered questions and profound frustration. You might feel pure agony in your back, knees, or neck, yet your doctor looks at an MRI and tells you everything looks normal. Or perhaps you undergo surgery to fix a "broken" part, expecting relief, yet the pain remains or even worsens weeks later.
For centuries, medicine has operated on the Biomedical Model. This view treats the human body like a car or a clock. If a gear grinds or a piston knocks, we assume it is broken. We assume we must fix the hardware to stop the signal. In this view, pain is a direct line from tissue damage to the brain.
But the human body is biological, not mechanical. It is a living, adapting ecosystem. While the Biomedical Model works well for acute injuries (like a broken leg from a fall) it fails miserably when applied to chronic pain.
Current science supports the Biopsychosocial Model. This approach proves that the true causes of persistent pain are often invisible to standard X-rays and MRIs. There are chemical and electrical drivers working alongside structure to keep you in pain.
Understanding all three drivers is the first step toward getting your life back. When you realize your body is not broken, you can start the work of rebuilding your strength and returning to the activities you love.
Here is what is actually happening under the surface.
Driver 1: The "Broken Part" Myth (Structural)
We are conditioned to believe that pain equals tissue damage. If you see a bulging disc, a meniscus tear, or arthritis on a scan, you naturally assume it is the source of your misery. It seems logical: there is a "defect," so there must be pain.
Modern imaging studies challenge this assumption. "Abnormal" findings are frequently normal.
In a landmark systematic review published in the American Journal of Neuroradiology, researchers analyzed imaging data from over 3,000 individuals who had no back pain at all. They found that by age 50, approximately 80% of pain-free people exhibited "disk degeneration" on their scans. Even more surprising, nearly 40% had bulging discs yet felt nothing (Brinjikji et al., 2015).
Similar studies show the same patterns in knees and shoulders. Many professional athletes compete at the highest levels with "torn" rotator cuffs or menisci they don't even know they have.
These findings are like grey hair or wrinkles on the inside. They are signs of aging and life, not necessarily signs of injury or fragility.
This matters because believing you are fragile leads to fear. If you think your spine is crumbling, you will move stiffly and avoid activity. This inactivity weakens your muscles and stiffens your joints, which paradoxically causes more pain. When you understand that your structure is robust and capable of handling load, you can stop protecting yourself. You can start trusting your body again.
Driver 2: The Toxic Soup (Chemical)
If the structure is stable and strong, something else must be driving the signal. Often, the culprit is the invisible chemical environment surrounding your nerves.
Chronic pain often involves systemic inflammation. When your immune system stays on high alert due to relentless stress, poor diet, autoimmune issues, or lack of sleep, it releases signaling molecules called cytokines (such as TNF-α and IL-6).
Think of these chemicals like an acid bath for your nerves. In a healthy state, your nerves are like calm water. In an inflammatory state, they are boiling. This "toxic soup" irritates the nervous system and drastically lowers your pain threshold.
-
The Glial Trap: Your nervous system contains immune cells called glia. Their job is to support neurons and clean up debris. However, in chronic pain, these cells can get stuck in an active state. They become overprotective, pumping out inflammatory chemicals to guard the area. This creates a hostile environment that keeps nerves sensitive long after an injury heals.
-
The Stress Connection: High stress levels disrupt cortisol regulation. Cortisol is your body's natural fire extinguisher for inflammation. When stress is chronic, this mechanism fails. Emotional stress physically alters your blood chemistry to maintain pain sensitivity.
You have the power to change this internal environment. It is not about a quick fix, but about consistent lifestyle shifts. Improving sleep quality, managing daily stress, and eating nutrient-dense foods can cool this chemical heat and soothe your irritated nerves.
Driver 3: The Software Bug (Electrical)
The most potent driver is arguably Electrical. This refers to how your nervous system processes and interprets signals, a phenomenon known as Central Sensitization.
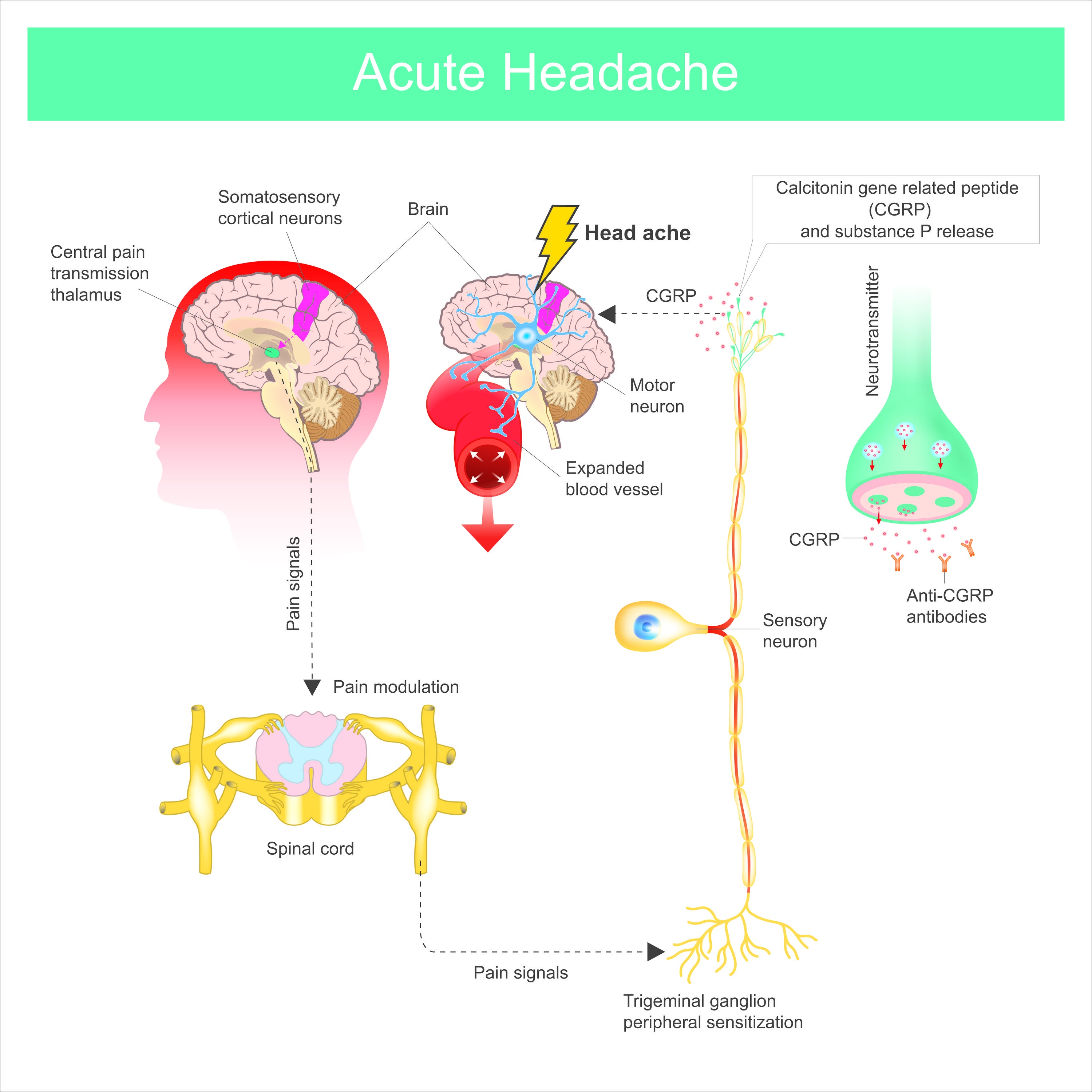
Dr. Clifford Woolf describes this as a shift in the central nervous system where neurons become hyperexcitable. Imagine your nervous system has a volume knob. In a healthy person, the volume sits at a 3. If you bump your knee, it spikes to a 6, then settles back down. In chronic pain, the chemical drivers and constant input turn that baseline volume up to a 10 (Woolf, 2011).
At this volume, the brain starts making mistakes. Normal inputs, like the light touch of a shirt, mild temperature changes, or simple movement, are processed as dangerous pain. This is a physiological malfunction in the electrical signaling of the spinal cord and brain.
The alarm system is malfunctioning. The house is not on fire, but the alarm is ringing at full volume.
This happens because of neuroplasticity—the brain's ability to change. Your brain gets "good" at what it practices. If it practices processing pain signals every day, it becomes more efficient at producing pain. The map of your body in your brain can even become "smudged," making it hard to pinpoint exactly where the pain is coming from, leading to spreading aches.
You can retrain this system. Through graded exposure to movement and visualization, you teach the brain that the signal is a false alarm and that movement is safe.
The Psychological Factor: Fear Drives the Cycle
Pain is not "all in your head," but your brain's prediction of danger fuels the fire.
Researchers Vlaeyen and Linton developed the Fear-Avoidance Model.

Their research highlights that fear of movement (kinesiophobia) and catastrophizing act as accelerants for pain (Vlaeyen & Linton, 2000).
If your brain expects movement to hurt, it generates pain signals before you even move to protect you. You might tense your muscles in anticipation, bracing for impact. This "guarding" alters your natural movement patterns, creates tension, and increases load on tissues.
This fear keeps the nervous system on high alert. It reinforces the Electrical volume knob and maintains the Chemical inflammation. It creates a self-fulfilling prophecy where the fear of pain leads to behaviors that guarantee pain.
Breaking this cycle requires courage. It requires moving even when you are uncertain. It means engaging in activity not because the pain is gone, but because you know the activity is safe.
Putting It All Together
These drivers feed each other in a continuous loop. A minor structural issue causes inflammation. Stress about the pain revs up the nervous system. Fear of movement locks it all in place.
You are not stuck this way. Your nervous system is plastic, meaning it can change.
-
Cool the Chemical: Prioritize sleep and stress management to lower systemic inflammation. Treat your body like a garden that needs the right soil to heal.
-
Rewire the Electrical: Use graded movement to show your brain that activity is safe. Start small and slowly build up.
-
Calm the Prediction: Challenge your fear. Remind yourself that "Hurt does not equal Harm." Soreness is often a sign of tissue adapting, not failing.
You are capable of more than you realize. The findings on your MRI do not dictate your future. By addressing the invisible drivers, you can return to sports, play with your kids, and handle daily life with confidence. The path out of pain is not about fixing a broken part; it is about building a resilient human.
Ready to Look Beyond the X-Ray?
If traditional treatments have failed you, it is likely because they only targeted the structure while ignoring the chemical and electrical drivers keeping you in pain. At 417 Performance, we do not just treat the scan; we treat the whole person.
Schedule your evaluation today to identify exactly which drivers are holding you back and build a comprehensive plan to get you back to high-level performance.
Sources
-
Brinjikji, W., et al. (2015). Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. American Journal of Neuroradiology, 36(4), 811-816.
-
Woolf, C. J. (2011). Central sensitization: Implications for the diagnosis and treatment of pain. Pain, 152(3 Suppl), S2–S15.
-
Vlaeyen, J. W., & Linton, S. J. (2000). Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain, 85(3), 317-332.
.jpg)


.png)